
The Knives Are Out For The Public Option (William Chirolas)
Categories
 We should oppose a fake
reform that fails to include a genuine public option. The let down of
no bill will be less than the let down of a GOP plan passed by
Democrats.
We should oppose a fake
reform that fails to include a genuine public option. The let down of
no bill will be less than the let down of a GOP plan passed by
Democrats.
William Chirolas -- World News Trust
June 7, 2009 -- The knives are out for the public option. Dear sweet Olympia Snowe, Republican, well-respected, and considered non-partisan, is selling herself as a cover for Democrats.
Thursday, June 4, Snowe held a private gathering of members of Congress and their staff to discuss the proposals of pharmaceutical (11 percent of the nation's heath bill) and insurance companies.
She is pushing the "trigger" idea, which is actually no public option ever because there would be a trigger as to how much insurance companies must bring down healthcare costs and expand coverage that is set so low for keeping the public plan off that the effects of the welfare check to the insurance companies as to cost of medical delivery (the computerization of the industry) will take care of the required slowing down in the increase over the next few years, and the mandate requiring everyone to have coverage will automatically expand coverage. She's already gained the tentative support of several Democrats (including Ron Wyden and Thomas Carper).
Other kill-public-plan proposals are to break up the public option into small pieces under multiple regional third-party administrators that would have little or no bargaining leverage (or the equivalent of setting up one in each state since buying the state legislature is seen as not a tough job for the insurance companies, many state reps being former insurance employees), or to bind the public plan not to the Senator Schumer fair competition rules, but to rules making the public plan charge the same as private insurers so as to have no competitive pressure. Like Bernie Sanders, Eric Massa, and John Conyers, we should oppose a fake reform that fails to include a genuine public option. The let down of no bill will be less than the let down of a GOP plan passed by Democrats.
If one needs a refresh on the issues, PBS at http://www.pbs.org/video/video/1050712790/subject/957383245 is not bad. Then go to http://www.usa.gov/Contact/Elected.shtml and find your elected officials (by zip code) and write to them that you want any health care reform bill to include a "full public option", without any of the triggers proposed by Sen. Snowe. For those that want to take direct action against there is a Defeat Baucus campaign at https://www.thedatabank.com/dpg/309/donate.asp?formid=meet&c=8161321
Right now we get none of the benefits of a government-managed plan (such as negotiated fees for services and for prescriptions) and all of the downsides as we as taxpayers get our pockets lightened by 8 percent of our families’ 2009 health care premiums -- $1,100 because our system doesn’t provide continuous coverage for all http://www.americanprogressaction.org/issues/2009/03/cost_shift.html -- as we pay for the medical care of the uninsured (a nearly $100 billion per year cost for what is often for preventable diseases or diseases that physicians could treat more efficiently with earlier diagnosis." (see http://www.nchc.org/facts/coverage.shtml). Other Western European countries seem to always record provide better outcomes at half the cost (or less) of U.S. health care). Meanwhile medical bills underlie 60 percent of U.S. bankruptcies as noted at http://www.reuters.com/article/newsOne/idUSTRE5530Y020090604, as U.S. Doctors support universal health care as noted at http://www.reuters.com/article/latestCrisis/idUSN31432035 where the journal Annals of Internal Medicine reports that of more than 2,000 doctors surveyed, 59 percent said they support legislation to establish a national health insurance program, while 32 percent said they opposed it.
The garbage that there can be no "fair competition rules" because the public plan has a line to the Treasury ignores the current insurance company overcharge up front followed by "claims underwriting" (denying claims you'd think the language of the policy said you were covered for, or delaying the approving new treatment or the payment of old until you are dead and there is no need for further procedures and a less interested person is asking the insurance company for money). The current insurance company no-regulations-on-price-or-performance model makes a mockery of the idea that "competition" always leads to improved delivery and quality of products and services, at lower cost to the consumer. That is exactly the opposite of what is happening in the insurance-based model adopted by the United States. We've already got examples to draw from -- Medicare and VA hospitals -- that show us what can be done with limited dollars. One does not see insurance companies wanted to take over the Medicare and VA -- that is not unless they can get their 10 percent of Medicare Cost additional welfare check -- the one they now get when they "compete" with Medicare.
The “American Health Choices Act”) has been circulated (6-05 DRAFT) to allow the members to suggest changes before the bill goes to mark-up.
PRIVATE INSURANCE MARKET REFORMS:
--Eliminates health status rating
--Requires guaranteed issue and renewability
--Requires all insurers to report MLRs (Loss Ratio is a value of premium concept that is just the ratio of the claims paid to the premiums collected - thereby exposing overhead and profit) to the Secretary (private insurers would have to pay out a specified percentage of their premium revenues in benefits).
--Requires coverage of certain preventive services
--Increases the age at which dependents are required to be offered coverage to 26
--Prohibits annual or lifetime limits on coverage
STATE-BASED INSURANCE GATEWAYS:
--Provides grants to states to create “gateways” (discussed below) through which individuals and small businesses may purchase insurance
--Provides reinsurance funding for plans participating in the gateway
--Establishes a Medical Advisory Council that will define, among other things, “essential health care benefits” that gateway plans must offer and “minimum qualifying coverage” that individuals must purchase
--For states that do not initially adopt the reforms in the bill, the insurance market provisions of the American Health Choices Act would automatically apply
--Would establish (but this draft leaves blank) the benefit levels (coinsurance, etc.) that gateway plans must adopt
--Would establish (but left blank) minimum MLRs (again the loss ratios - percent of premium paid to insureds as opposed to overhead and profit) for gateway plans
--Provides subsidies up to 500% of FPL (this poverty level reference seems to mean $110,000 for a family of four) for the purchase of insurance
--Establishes small business credits for purchasing insurance (with the size of “small business” to be determined)
--Gateway plans made available to employees if their employer does not offer “qualified coverage” or if plan options are not “affordable” (terms to be defined)
--Includes a play-or-pay employer mandate and possibly an individual mandate (perhaps similar to the Massachusetts pay or play rules that Republican Governor Romey approved)
--Establishes HIT program for electronic enrollment in gateway plans
OTHER PROVISIONS:
--Increases Medicaid eligibility to 150% of FPL (150% of the poverty level - $33,075 - but the eligibility change is in very general language since the Finance Committee has jurisdiction over the program)
--Establishes a Community Living Assistance Support Service (CLASS) for the 10 million disabled, homebound, and institutionalized individuals
--Provides a credit for employers who auto-enroll their employees into offered health plans
--Suggests new coverage options for retirees which I hope is a reference to a Medicare buy-in
--And appears to provide a public plan option, with the Secretary of Health and Human services establishing the new government-sponsored plan, which would compete directly with private insurers. The new government-run program would pay doctors and hospitals at Medicare rates, plus 10 percent.
People would be exempt from the pay-or-play penalties if “affordable health care coverage is not available” or if the premium payments would cause “an exceptional financial hardship” just as Obama recommended. The Secretary of Health and Human services would establish a panel of experts, the Medical Advisory Council, to recommend a minimum package of insurance benefits where the “essential benefits” would include doctors’ services, hospital care, maternity and newborn care, prescription drugs and mental health and substance abuse services. If Congress did not disapprove the recommendations, insurers would generally have to provide the benefits. Private group or individual insurance company health plan would be required to provided coverage for children and their parents with the child's coverage inforce through age 26 unless no longer "dependent".
Grants would be made to the states to establish insurance marketplaces or exchanges called "health benefit gateways" that would put out information about premiums and benefits, and assist people in enrolling -- again similar to the current Massachusetts Plan. Reinsurance -- the sharing of the risk that one insurer enrolled more sick persons than the others -- would be subsidized by subsidy payments from the government, with the government doing the administration of the reinsurance, moving the reinsurance premium from the companies that enrolled mainly healthy persons to those that enrolled the more sickly. All of this reinsurance of course is currently done by reinsurance insurance companies but would now be the responsibility of the government, with those reinsurance insurance companies no doubt doing the administrative services, the same way the insurance companies currently do the administrative services for Medicare Part B.
***
William Chirolas brings 40 years of real-world business experience in local, state, national, and international tax, pensions, and finance to the world of blogging. A graduate of MIT, he calls the Boston area home, except when visiting kids and grandkids.
-
CreatedSunday, June 07, 2009
-
Last modifiedWednesday, November 06, 2013
World Desk Activities

www.niemanlab.org/2024/04/inside-newsweek-ai-exper…

www.journalismfestival.com/programme/2024/reader-r…

Reader revenue beyond the English language – – International Journalism Festival
In the past few months, many news publishers in the US have announced layoffs. Others have tweaked or abandoned their paywalls and pursued more open models.…
phys.org/news/2024-04-surf-clams-coast-virginia-re…

Surf clams off the coast of Virginia reappear and rebound
The Atlantic surf clam, an economically valuable species that is the main ingredient in clam chowder and fried clam strips, has returned to Virginia waters…
medicalxpress.com/news/2024-04-antibiotics-reveal-…
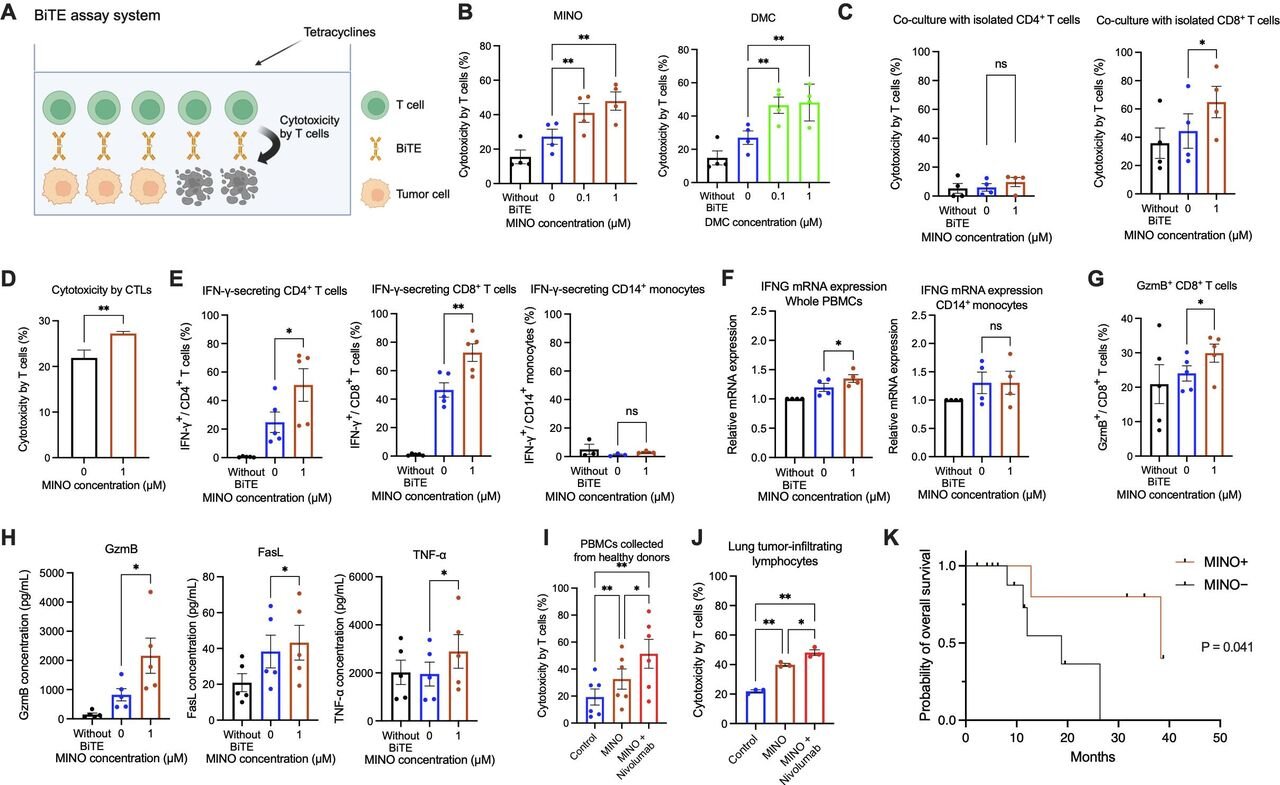
Antibiotics reveal a new way to fight cancer
Cancer cells grow and spread by hiding from the body's immune system. Immunotherapy allows the immune system to find and attack hidden cancer cells, helping…
phys.org/news/2024-04-crucial-quantum-internet.htm…
Crucial connection for 'quantum internet' made for the first time
Researchers have produced, stored, and retrieved quantum information for the first time, a critical step in quantum networking.
medicalxpress.com/news/2024-04-women-major-complic…

Women who experience major complications during pregnancy found to have increased risk of early death years later
A team of medical researchers from the University of Texas Health Science Center, in the U.S., and Lund University, in Sweden, has found via study…
medicalxpress.com/news/2024-04-common-hiv-treatmen…
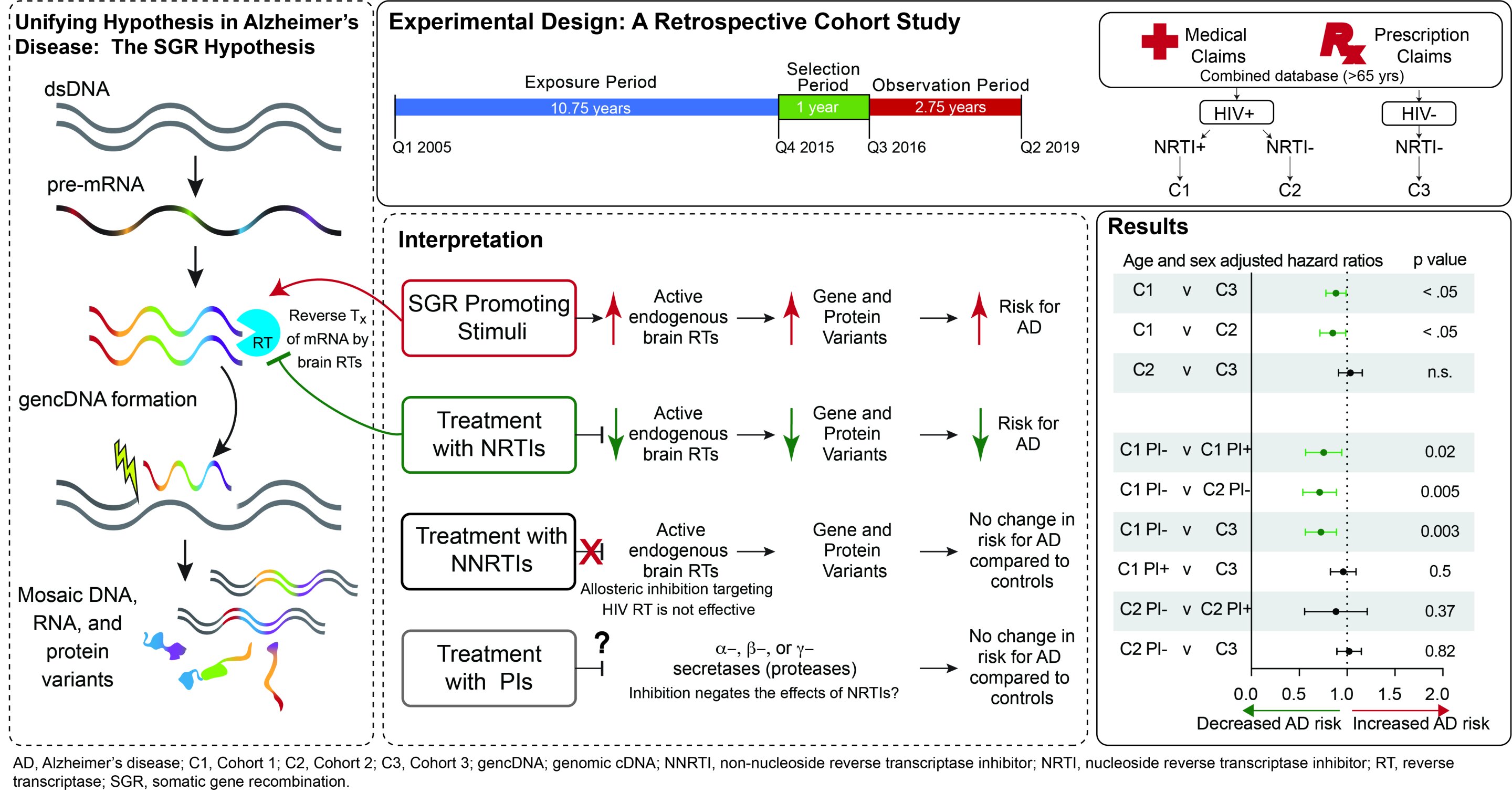
Common HIV treatments may aid Alzheimer's disease patients
Alzheimer's disease (AD) currently afflicts nearly seven million people in the U.S. With this number expected to grow to nearly 13 million by 2050, the…
medicalxpress.com/news/2024-04-adolescent-stress-p…

Study suggests adolescent stress may raise risk of postpartum depression in adults
In a new study, a Johns Hopkins Medicine-led research team reports that social stress during adolescence in female mice later results in prolonged elevation of…
medicalxpress.com/news/2024-04-positive-effect-mel…
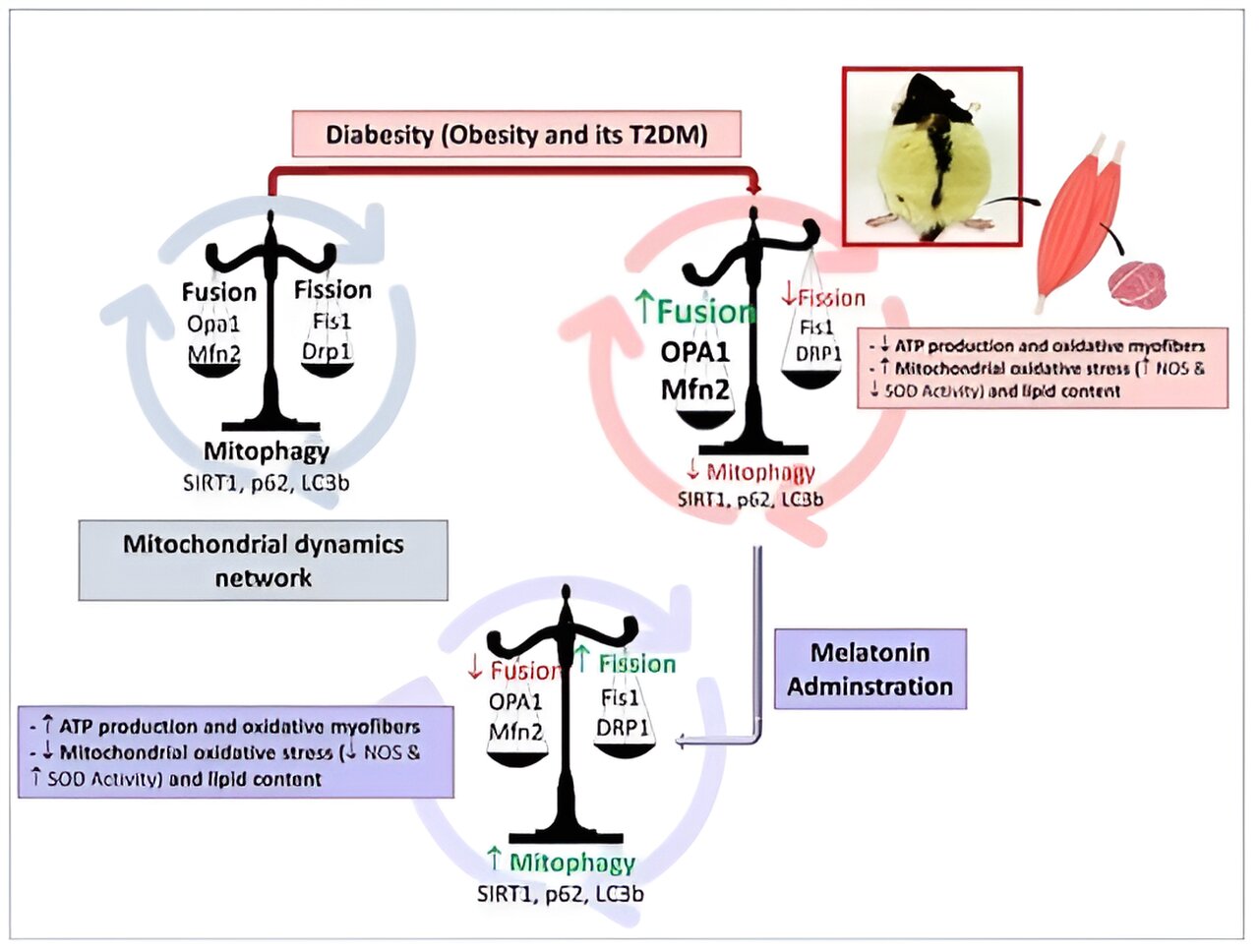
Researchers demonstrate the positive effect of melatonin in the prevention of obesity
Two international studies led by the University of Granada (UGR) have confirmed that melatonin helps prevent obesity. In addition, its effects are positive against visceral…
medicalxpress.com/news/2024-04-fecal-transplants-p…
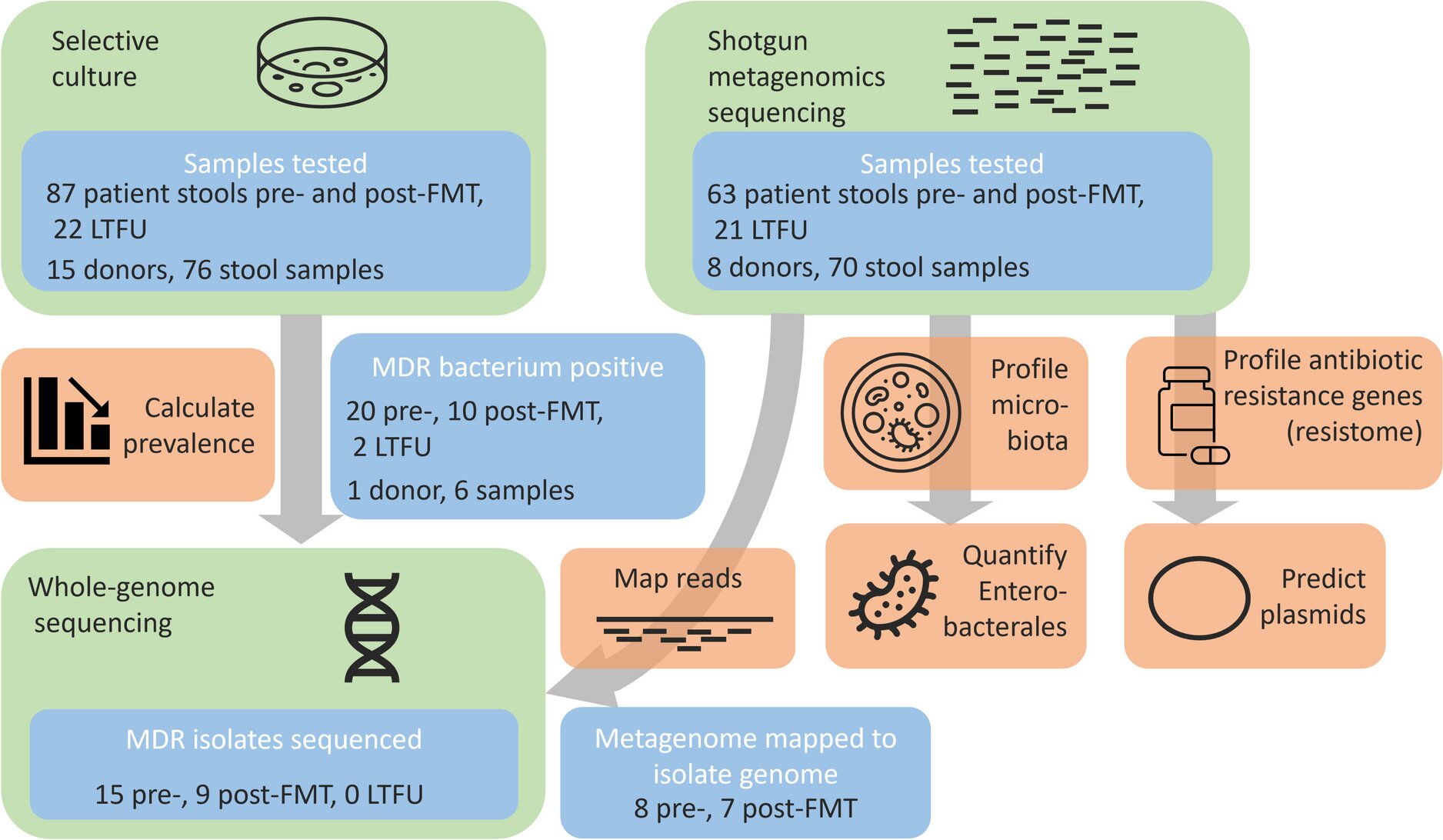
Researchers conclude fecal transplants can rid patients of resistant gut bacteria
Transferring fecal microbiota from healthy donors to the intestines of chronically ill people has beneficial effects on these recipients' gut bacteria, also in the longer…
Latest Stories







Electronic Frontier Foundation
-
Internet Service Providers Plan to Subvert Net Neutrality. Don’t Let Them
April 19, 2024
-
EFF, Human Rights Organizations Call for Urgent Action in Case of Alaa Abd El Fattah
April 19, 2024
-
Congress: Don't Let Anyone Own The Law
April 19, 2024
-
Two Years Post-Roe: A Better Understanding of Digital Threats
April 18, 2024
The Intercept
-
Since October, Sen. John Fetterman Has Been Building a Roster of Republican Donors
April 19, 2024
-
Idaho Goes to the Supreme Court to Argue That Pregnant People Are Second-Class Citizens
April 19, 2024
-
U.S. Troops in Niger Say They’re “Stranded” and Can’t Get Mail, Medicine
April 18, 2024
-
Columbia Suspends Ilhan Omar’s Daughter One Day After Omar Grilled School Administrators
April 18, 2024
VTDigger
-
LAST DAY: 3X your gift and send a children’s book
April 19, 2024
-
Roger Ormiston
April 19, 2024
-
Final Reading: In the Vermont Senate, Friday afternoons are for budget building
April 19, 2024
-
Becca Balint to vote in favor of aid to Ukraine, against aid to Israel
April 19, 2024
Mountain Times -- Central Vermont
-
The Mountain Times – Volume 51, Number 16 – April 17-23, 2024
April 17, 2024
-
Weekly Horoscope: April 17-23, 2024
April 17, 2024
-
Bookstock cancels summer event after 14 years
April 17, 2024
-
Crêpe breakfast tradition at sport hill
April 17, 2024
